AIFiM M
Italian Association of Physiotherapists for the Study and Development of the Mezieres Method
Advanced Institute of Neuro-Myo-Fascial Biomechanics
AIFiMM Provider ECM n° 1701
The only Mezieres school to have been directly recognized by the Italian Ministry of Health, becoming ECM Provider n° 1701


Systemic and Analytical Musculoskeletal Biomechanics – Online Course
Physics-based clinical model | Based on the Mézières Method
Subscribe to the courseOfficial Certifications — UK & USA
Official Evaluation — The CPD Certification Service (UK):
"An advanced online course providing rehabilitation professionals with a scientifically grounded model for assessing and treating musculoskeletal dysfunctions through systemic biomechanics.
Based on the principles of the Mézières Method, it integrates physics, myofascial chain analysis, and vector-based muscle assessment to identify primary and secondary shortenings, optimize joint alignment, and restore functional balance.
Includes 32h of video lessons and 6h of reading materials, with demonstrations, case studies, and diagnostic tools."
|

Officially Certified in UK & USA |
– 38 CPD hours (UK, The CPD Certification Service – Provider No. 21418) – 45 contact hours / 4.5 CEU (Florida, PT & PTA – CE Broker ID 50-54885) |
On-Demand Video Course |
All content is pre-recorded and available 24/7 for 12 months. No scheduled webinars or live sessions – learn at your own pace, on your own schedule. |
Watch a Free 2-Hour Sample Lesson |
👉 Click here to open the enrollment page and scroll to the bottom to access the free lesson. |
Trusted by over 6,000 physiotherapists |
Official ECM evaluations (Italy, Ministry of Health 1997–2024):
|
38 hours of structured online training |
32h HD video + 6h guided readings, with manual and 25+ downloadable resources |
For physiotherapists, osteopaths, and rehabilitation professionals |
Designed for licensed clinicians seeking advanced tools in analitical and systemic MSK biomechanics |
International recognition |
CPD certification is recognized in many European countries, Australia, and New Zealand. In Canada and other Commonwealth countries, it is often recognized or accepted depending on local regulations |
The Mézières Method: A Revolutionary Discovery
In 1947, while treating a patient with thoracic hyperkyphosis, French physiotherapist Françoise Mézières observed an unexpected phenomenon that would change her approach to rehabilitation:
Attempting to correct the patient's shoulders while lying supine, a marked lumbar hyperlordosis immediately appeared. Blocking this lordosis with knee flexion, the hyperlordosis instantly shifted to the cervical level.
From this simple observation, Mézières deduced three revolutionary principles:
1. Dorsal muscles behave as a single muscle Isolated muscles do not exist; there are muscular chains where every local action affects the entire system.
2. These muscles progressively tend to shorten, not to weaken Contrary to the knowledge of the time, muscles develop progressive structural shortenings that alter joint geometry.
3. These shortenings are the cause of most dysmorphisms and orthopedic pathologies It is not the skeleton that determines posture, but shortened musculature that deforms the skeleton.
Summary of articles written by Francoise Mezieres
What makes this approach different:
• Does not work on muscle strengthening, but on reducing deforming tensions The problem is not weakness, but excess tension in shortened muscles.
• Identifies which muscle shortenings generate joint misalignments Even distant from symptoms: knee valgus may depend on psoas-diaphragm system shortenings.
• Explains chronic, migrating, or treatment-resistant cases through systemic analysis The local symptom is often the expression of a global imbalance in muscular chains.
• Applies to most orthopedic pathologies sustained by biomechanical alterations From shoulder impingement to chronic low back pain, from scoliosis to joint conflicts.
A European Clinical Tradition, Now Systematized for International Practice
Mézières' observations, initially empirical, anticipated by decades principles that today find explanation in applied physics and complex systems theory.
For over 70 years, this method has been a cornerstone of European physiotherapy — but remained largely unknown in English-speaking countries due to limited translation and systematization.
AIFiMM instructors, trained directly with Mézières, have spent 30 years rationalizing this clinical heritage through vector analysis, developing an interpretative model based on:
• Vector analysis of muscular forces acting on the skeletal system
• Calculation of force resultants that determine articular axial deviations
• Direct correlations between specific muscular shortenings and measurable joint alterations (knee valgus, anterior humeral head displacement, vertebral rotations, etc.)
The course provides tools to:
• Identify dominant muscular vectors in joint alterations
• Build clinical reasoning based on verifiable biomechanical principles
• Develop therapeutic strategies that act on mechanical causes, not just symptoms
An approach that integrates the clinical efficacy of the original method with a biomechanical rationalization that allows explaining and verifying every therapeutic choice.
Course Accessibility
The course does not require prior knowledge of advanced physics or mathematics.
Biomechanical principles are introduced gradually with practical clinical examples, starting from patient observation to arrive at understanding the underlying physical laws.
Most participants come from standard training backgrounds and progressively acquire vector analysis tools through supervised practice and real cases.
Clinical Application
The method is particularly effective for:
- Chronic musculoskeletal symptoms unresponsive to conventional treatments
- Pain that alternates or migrates between body regions
- Recurrent issues without clear traumatic cause
- Persistent functional limitations post-surgery
- Most orthopedic pathologies sustained by muscular biomechanical alterations
The biomechanical approach provides tools to identify mechanical primary causes through vector analysis of muscular forces — going beyond the local symptom to resolve the biomechanical conflict that generates it.
The method is based on treating simultaneously the local problem (vectorial rebalancing of the symptomatic district) and distant joint alterations. Each local intervention is constantly evaluated for its effects on all joints, to avoid improvements in one district creating compensations in others.
The Phenomenon of Muscle Shortening: From Physics to Clinical Practice
Scientific Insight
Muscle shortening is not a neurological phenomenon but a physical one.
The connective component of muscle, with an elasticity coefficient lower than 1, behaves like an imperfect elastic body: after contraction, part of the deformation remains.
This residual tension accumulates over time, increasing internal resistance and reducing the muscle’s ability to produce effective mechanical work.
Understanding this principle is essential to explain why chronic stiffness persists even in the absence of pathology — and how it can be reversed through precise vector-based treatment.
The Basic Principle
In the absence of specific pathologies, clinical practice reveals that muscles progressively tend to shorten their length. The connective components, having an elasticity coefficient less than 1, maintain residual deformations proportional to the applied force and application time.
The skeleton, lacking autonomous motor capacity, suffers the consequences of muscular forces: alterations of joint axes, asymmetric load concentration, intra-articular conflicts, and deviations of the vertebral sinusoid. On the dynamic level, while resistant force increases, Work and Power decrease: the shortened muscle dissipates energy to overcome internal resistances before producing useful movement.
Segmental Analysis
In the course, muscles are not considered in their anatomical reality but as force lines to which vector decomposition is applied to identify their deforming action on joint axes and on both frontal and sagittal deviations of the vertebral sinusoid.
The parallelogram rule allows calculation of resultants, identification of muscles responsible for alterations, and determination of targeted intervention for restoration of physiological joint sequence. Each joint is examined in its vector components to understand mechanical conflicts and apply specific treatment. The spine, analyzed three-dimensionally, reveals calculable deviations that can be corrected through rebalancing of identified muscular forces.
Systemic Interpretation
The symptom can be local or referred. Through segmental innervation, vertebral disorders manifest in peripheral districts. Visceral, neurological, stomatognathic problems, etc. can trigger secondary muscular shortenings with symptoms distant from the primary dysfunction, necessitating a multi-disciplinary approach. Dermatomeric charts and organ-vertebra mapping allow tracing the path from symptom to cause.
The Therapeutic Approach
Assessment: Static examination to identify axis alterations through vector analysis. Dynamic examination for limitations and compensations. Exclusion tests to distinguish primary from secondary problems.
Treatment: Reduction of excess tension in shortened muscles. Differentiated techniques for contractile and connective components, respecting tissue physical properties. Objective: decrease resistant force in favor of Work and Power.
Verification: Immediate therapeutic test. Stable correction indicates resolution of mechanical conflict. Persistence suggests unresolved systemic causes.
The course provides tools to translate clinical observation into vector analysis and act on musculoskeletal pathologies both analytically and systemically.
Course Program: Your Complete Learning Pathway
Here's a concise overview of the course structure, blending theory, live demonstrations, and clinical applications:
-
Theoretical Foundations and Assessment (videos 1–4 – 8h 30min)
Causes of muscular shortening, concepts of Resistant Force and Working Force, vector analysis applied to the muscular system, biomechanical principles, effects of isometric contraction in maximum physiological or relative elongation of the muscle fiber as a therapeutic tool, three-dimensional visual and palpatory assessment of the patient, manual techniques, and modalities of active work performed by the patient. Theory and practical demonstrations.
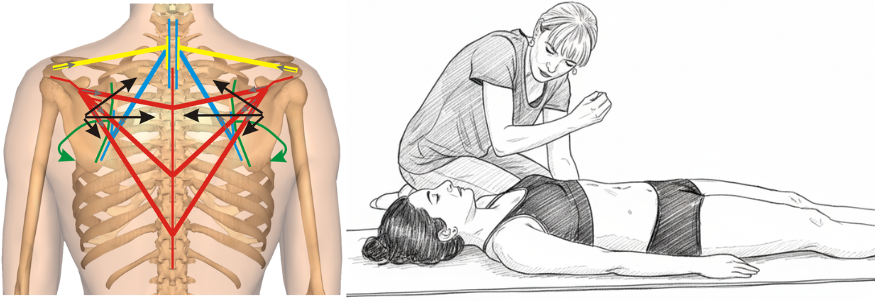
The core innovation: transforming anatomical muscles into force vectors to predict their mechanical effects. Left: Vector analysis reveals how shortened muscles create predictable force patterns affecting scapular positioning. Right: Clinical application where the therapist uses this vector understanding to guide treatment, working with therapeutic breathing to reduce resistant forces.
-
Sagittal Plane Corrections (videos 5–6 – 3h 55min)
Evaluation and corrective treatment, both segmental and systemic, of the cranio-vertebro-sacral system in the sagittal plane. Theory and practical demonstrations.
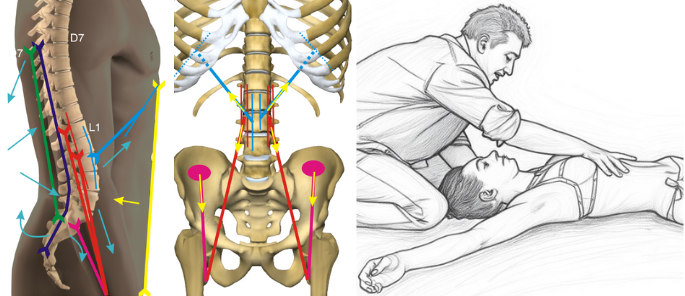
Vector analysis of forces acting between D7 and sacrum with their resultant force lines. Clinical application exemplifies how vector understanding guides therapeutic positioning - one example from the comprehensive toolkit of sagittal techniques presented in the course.
-
Frontal and Rotational Plane Corrections (videos 7–9 – 5h 51min)
Evaluation and corrective treatment, both segmental and systemic, of the cranio-vertebro-sacral system in the frontal plane; evaluation and treatment of upper limb pathologies and their connection with vertebral, costal, and hyoid dysfunctions. Theory and practical demonstrations.
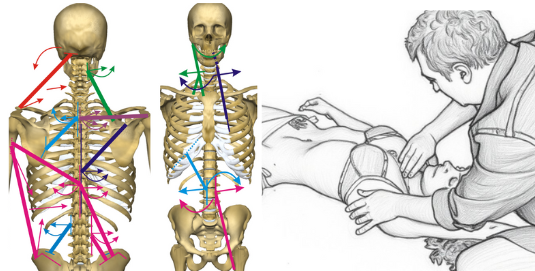
Vector analysis in the frontal plane reveals asymmetries and rotational patterns of the cranio-vertebro-pelvic system. Mechanical connections between upper limb and vertebro-costal complex guide integrated treatment - one of the specific approaches for frontal and rotational dysfunctions.
-
Lower Limbs and Specific Techniques (videos 10–12 – 5h 36min)
Evaluation and treatment, analytical and systemic, of lower limb pathologies and their relationship with vertebral dysfunctions. Theory and practical demonstrations.
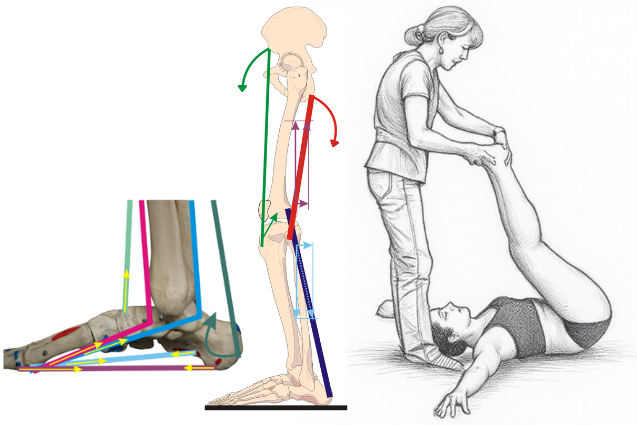
Vector representation of force lines acting on medial plantar arch and lower limb, with example of their treatment. These mechanical relationships enable both local and systemic therapeutic interventions.
-
Specific Districts (videos 13–15 – 5h)
Distinction between primary muscular problems and those secondary to structural alterations from other systems. Evaluation and treatment of TMJ disorders and the multidisciplinary approach, dynamic analysis and identification/treatment of altered patterns, treatment of humeral and sternoclavicular subluxations. Theory and practical demonstrations.
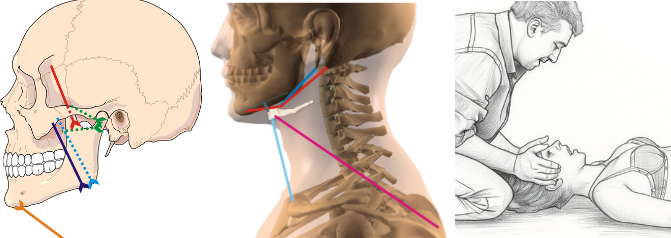
Vector analysis of temporomandibular joint, hyoid bone and cervical connections, with specific clinical application. Understanding these anatomical relationships determines whether direct treatment or multidisciplinary referral is indicated.
-
Clinical Reasoning (videos 16–18 – 3h 04min)
The symptom as an expression of a local or referred problem; from static and dynamic objective examination to treatment planning. Scoliosis: evaluation and treatment. Theory and practical demonstrations.
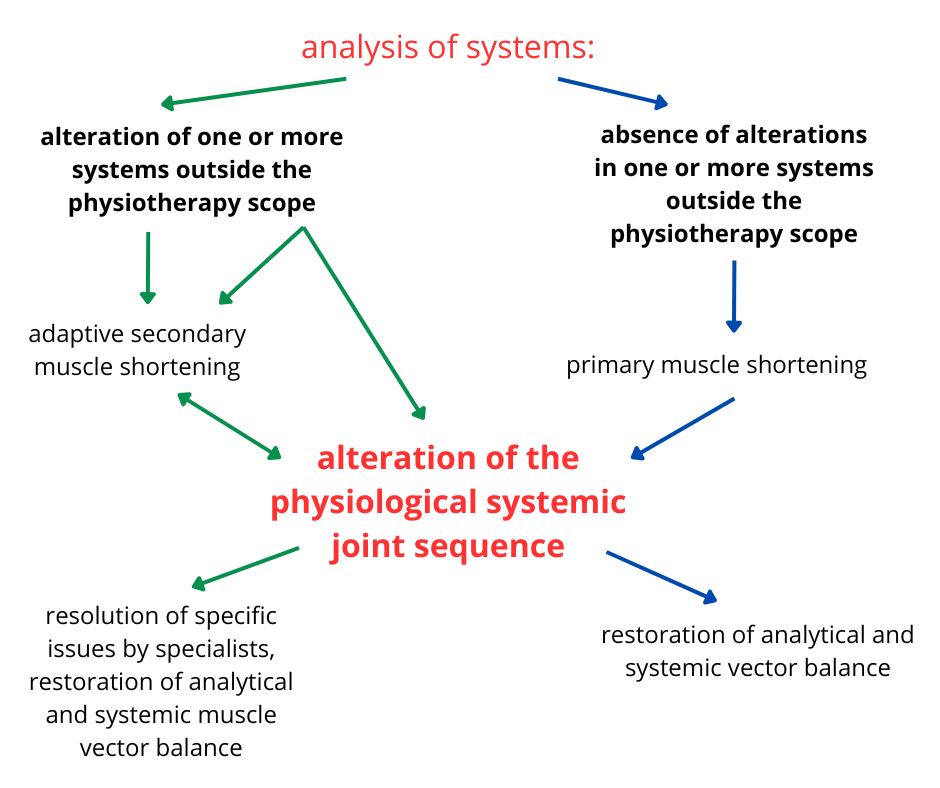
Systemic clinical reasoning: from systems analysis to treatment planning. The diagram illustrates the decision-making process for distinguishing between primary muscle shortenings (directly treatable) and secondary ones (requiring multidisciplinary approach), guiding optimal therapeutic strategy.
📌 Each video includes theoretical lessons, live demonstrations, and downloadable PDF materials. Download full program
When and How This Method Applies to Clinical Practice
Typical Clinical Presentations
The method is particularly effective for:
- Chronic symptoms unresponsive to conventional treatments
- Pain that alternates or migrates between body regions
- Recurrent issues without clear traumatic cause
- Persistent functional limitations post-surgery
Treatment Characteristics:
- Individual 60-minute sessions at weekly frequency
- Active approach based on guided isometric contractions in maximum elongation
- Not based on standardized protocols: each session requires continuous observation and adaptation
- Active patient participation, constantly guided by the therapist
- Documentable short-term results with long-term maintenance
Note: The online course provides theoretical foundations and demonstrates practical application through video. Direct hands-on practice should be organized independently or through supplementary in-person training.
What Makes This Approach Different
- Focus on reducing resistant force rather than strengthening weak muscles
- Treatment targets vectorially responsible muscles (which may also be distant from symptoms)
- Goal is correcting mechanical joint conflicts and restoring mobility through precise lengthening work
- Small percentage shortenings (1-2% of muscle length) require precise, progressive stimuli rather than forceful stretching
Expected Treatment Outcomes
Objective and subjective changes should be evident from the first sessions. When this does not occur, trained therapists systematically evaluate:
- Possible compensations in other body regions not initially identified
- Accuracy of the initial assessment of dominant vectors
- Presence of non-muscular primary causes (e.g., dental, visceral, visual, etc.) requiring multidisciplinary approach
- Psychosocial factors that may influence symptom maintenance
As with any evidence-based therapeutic approach, approximately 15% of patients do not respond to treatment - this reflects normal biological variability and the complexity of the therapeutic relationship.
Precautions and Contraindications
The method follows standard physiotherapy contraindications based on clinical common sense. Special caution is required in conditions such as:
- Acute phases (where pharmacological approach takes priority)
- First trimester of pregnancy
- Extensive spinal stabilizations
- Conditions where joint mobility is structurally limited
The trained therapist evaluates each case individually, adapting or deferring treatment as clinically appropriate.
Why this model changes your practice
This course introduces a biomechanical framework that explains musculoskeletal dysfunctions through predictable physical laws.
Not pre-packaged protocols, but mechanical logic: forces that add up, oppose each other, and reorganize the system.
📌 Clear examples
• When the psoas shortens structurally, it drags the lumbar vertebrae into lordosis.
The abdominals, although active, cannot counter this traction: it is not a matter of “strength” or “weakness,” but of vector mechanics.
• An engineer calculates loads before building a bridge; they don’t build a hundred bridges to see which ones collapse.
Likewise, vector analysis shows which muscle alters alignment and in which direction.
• Knee pain without evident axial deviations can be the metameric projection of an L3–L4 compression: treating the muscles responsible for that upstream compression may resolve the symptom more effectively than treating the knee locally.
📌 From principles to clinical practice
• Identify which muscle to treat first
• Choose the correct patient positioning
• Sequence isometric contractions
• Use guided exhalation to facilitate release
📌 The two pillars of the model
- Structural muscle shortening
A muscle is composed of:
- a contractile component (elastic, always returns to its initial length),
- a connective component (rigid, tends to maintain deformation).
When the connective component is subjected to prolonged tension, it remodels and maintains the shortening.
This generates a Resistant Force (RF) that constantly acts as deforming tension and subtracts part of the Working Force (WF) available for movement.
👉 The muscle does not simply become “weak”: it becomes inefficient, because it consumes energy internally instead of transferring it to movement.
- Vector analysis
Muscles never push: they act only by traction.
Each muscle can be represented as a vector with three elements: magnitude, direction, sense.
Joint geometry results from the sum of muscular vectors.
👉 Even a minimal shortening (1–2%) of a dominant vector can produce macroscopic consequences on joint alignment, disc compression, and load distribution.
📌 Integration with EBM
This model does not replace evidence-based practice: it complements it.
• Statistics tell us what works on average.
• Physics explains why and how it works in the individual patient.
👉 Combining data with causal logic strengthens clinical reasoning.
🔎 The three guiding principles
- Muscle as a force vector: when connective tissue shortens, the vector remains permanently active.
- Loss of physiological joint sequencing: dominant vectors disorganize alignment and increase compression.
- Systemic compensation: the body preserves function by adapting at a distance; if the primary cause is not treated, symptoms recur or migrate.
TWO CLINICAL SCENARIOS: WHEN THE METHOD WORKS
After reviewing the general principles, we now move to the core of clinical practice: when the biomechanical model is resolutive and when it must be integrated with other disciplines.
📌 The key concept: Resistant Force (RF) and Working Force (WF)
A muscle does not generate only useful force for movement. Each contraction divides into two components:
- Working Force (WF) → the effective portion, producing functional movement.
- Resistant Force (RF) → the “parasitic” portion, generated by shortened connective tissue, constantly pulling as mechanical tension.
When RF > WF, the muscle ceases to be an efficient motor and becomes a deforming factor: it alters joint axes, increases compression, and generates conflicts.
⚖️ Scenario 1 – Primary muscular origin
- No congenital or acquired pathologies are present.
- The mechanical conflict arises from structural muscular shortenings.
- Reducing RF through isometric contractions in maximum elongation leads to:
static rebalancing of the joints, automatic recovery of dynamic function.
🔹 Local example (simplified): in some cases of scapulohumeral impingement without major bone alterations, the conflict between the humeral head and the coracoacromial arch is favored by two dominant vectors:
• shortened scapular adductors → scapula displaced backward
• dominant internal rotators → humeral head pushed forward
The reduction of the subacromial space is therefore the effect of a vector imbalance.
🔹 Distant example (simplified): knee pain without axial deviations may represent the metameric projection of an L3–L4 compression. In this case, the most effective intervention is not on the knee itself but on the muscles responsible for the lumbar compression.
⚖️ Scenario 2 – Primary structural origin
- In this case, the cause is not muscular but external (skeletal, stomatognathic, visceral, visual alterations, etc.).
- Muscles compensate, generating secondary imbalances.
- Biomechanical treatment can reduce symptoms, but only transiently.
- A multidisciplinary approach is required to correct the primary matrix.
🔹 Example (simplified): recurrent cervical pain may be sustained by a vertebral rotation maintained by shortened scalenes and levator scapulae. Biomechanical treatment reduces pain, but the benefit is unstable until the stomatognathic problem that drives the rotation is corrected.
📌 Comparative synthesis
- Scenario 1 → muscle is the cause → biomechanical treatment can be resolutive.
- Scenario 2 → muscle is an adaptation → biomechanical treatment is complementary.
🔬 In-depth: vector logic in clinical practice
- Muscles act as traction forces, representable as vectors.
- The position of bones in space is the sum of these vectors.
- Some vector dominances are predictable: for example, at the humerus level, internal rotators have vector dominance over external rotators.
- Consequently, it is also predictable in which direction a joint axis will tend to alter.
- 👉 It is the gap between how a joint sequence is altered and how it should be physiologically that determines whether pathology develops.
💡 Elective clinical techniques
The primary technique for reducing RF is based on:
- isometric contractions in maximum physiological or relative elongation of the muscle fiber,
- maintained during prolonged active exhalation,
- with constant control of compensations by the therapist.
When direct isometric work is not possible, subdominant muscles are used as motors to lengthen dominant ones (e.g., the serratus anterior, by abducting the scapula, stretches the shortened scapular adductors).
In addition, specific manual and proprioceptive techniques are employed to ensure precision of therapeutic action.
👉 [Download full program – PDF]
START YOUR TRAINING
What you will learn in this course
📚 Core skills
-
Vector analysis
→ learn to identify the dominant muscles responsible for joint misalignments (e.g. the internal rotators of the humerus, which by vector dominance prevail over the external rotators and push the humeral head forward). -
Differential diagnosis
→ distinguish primary causes from secondary adaptations (e.g. knee pain without evident axial deviations that is actually the dermatomeric projection of an L3–L4 vertebral compression). -
System mapping
→ reconstruct the logical chain from symptom to origin, connecting distant districts through dermatomeric projections and myofascial chains. -
Therapeutic techniques
→ apply the elective technique: isometric contractions in maximum physiological or relative elongation of the muscle fiber, integrated with guided exhalation. When direct isometry is not possible, use subdominant muscles as motor agents to stretch dominant ones (e.g. the serratus anterior, abducting the scapula, stretches the scapular adductors). All with therapist control of compensations and integration of manual and proprioceptive techniques. -
Treatment sequencing
→ decide what to treat first and what to preserve, avoiding destabilization of the system through partial or isolated corrections.
💬 “Understanding vectors means knowing where to intervene and in what sequence.”
— Mauro Lastrico, PT
🎥 Structured training
🎥 Structured training
✓ 18 video modules (32 hours) + 6 hours of guided readings and downloadable materials
✓ On-demand access: available 24/7 for 12 months
✓ Live demonstrations with detailed biomechanical analysis on real patients
✓ Dedicated chat support with Mauro Lastrico and Laura Manni throughout your learning journey
✓ Complete textbook and all supplementary materials in English (PDF)
✓ Over 25 downloadable clinical resources
Instructors are available for clarifications, clinical doubts, and in-depth discussions throughout the entire course.
📌 Expected outcomes
• Ability to interpret complex symptoms through systemic biomechanics
• More precise and lasting therapeutic interventions
• Tools to integrate physical and vector-based logic into daily clinical practice
• Competence in distinguishing between primary causes and compensatory adaptations
📊 Who this is (and is not) for
Who this is for
- Suitable for all experience levels - from newly qualified to senior clinicians
- All concepts explained step-by-step with no prior knowledge of the method required
- Prerequisites: Basic knowledge of musculoskeletal anatomy and physiology
- For physiotherapists, osteopaths, and rehabilitation professionals seeking diagnostic and therapeutic tools grounded in biomechanics
- Not for you if you are looking for prefabricated routines or non-clinical education
- ❓ Mini EBM FAQ
• Does this replace evidence-based practice? No: it integrates it. Mechanical laws explain why and how in the individual patient.
• Do I need to calculate formulas? No: you will use practical clinical criteria (vector analysis, treatment sequencing).
• Is it immediately applicable? Yes: each module takes you step by step, from assessment to treatment.
• Has it already been clinically tested? Yes: the model originates from the work of Françoise Mézières (1947) and has been progressively systematized by AIFiMM. In Italy, AIFiMM courses have trained over 6,000 physiotherapists, with official ECM evaluations reported to the Italian Ministry of Health
Fees, access, and certification
💶 Course fee
- One-time payment: €610
- Or 2 installments of €305
- Secure payments via Stripe (credit/debit card)
- No hidden fees, no renewals
💻 Access
- Immediate after payment
- 12 months unlimited access
- HD streaming + complete PDF manual
🎓 Certification
- Digital certificate issued after course completion
- Granted upon passing the final test (20 multiple-choice questions)
- Delivered by email in PDF format at no extra cost
- Valid for:
- 38 CPD hours (UK) – The CPD Certification Service (Provider No. 21418)
- 45 contact hours / 4.5 CEU (USA, Florida) – CE Broker Provider ID 50-54885
AIFiMM and the instructors
📌 The institute
AIFiMM (Italian Association of Mézières Physiotherapists – Institute of Musculoskeletal Biomechanics) has been active since 1996, dedicated to clinical training in biomechanics.
• Officially accredited as: ECM (Italy), CPD (UK), CEU (USA)
• 27+ years of postgraduate education
• Over 300 courses delivered
• More than 6,000 physiotherapists trained directly
AIFiMM’s teaching model combines the tradition of historical Mézières (internationally spread since 1947) with a contemporary rationalization based on applied physics and vector analysis, developed and systematized in Italy.
📌 The instructors
- Mauro Lastrico, PT – over 40 years of clinical experience; trained directly with Françoise Mézières (Paris, 1988–89); author of Musculoskeletal Biomechanics and the Mézières Method (3rd ed., 2023); former lecturer at the University of Pisa; systematized Mézières’ insights into a physics-based clinical model. He has delivered over 300 courses, training more than 6,000 physiotherapists.
- Laura Manni, PT – over 40 years of clinical experience; trained with Françoise Mézières in France; co-developer of AIFiMM systemic assessment protocols; specialist in spinal dysfunctions and systemic compensations; recognized for making complex concepts immediately applicable.
📌 Teaching quality – Official ECM data (1997–2024, 6,147 evaluations submitted to the Italian Ministry of Health)
-
73% rated the topics very relevant, 26% relevant
-
71% rated overall educational quality excellent, 27% very good
-
78% rated the training very useful, 21% useful
-
75% rated the delivery of theoretical content excellent
-
77% rated the delivery of practical content excellent
-
76% rated responsiveness to student needs excellent
-
93% rated the balance between theory and practice adequate
-
87% rated the duration of the program adequate
-
Over 90% of participants reported they would recommend the course to a colleague (ECM official data, Ministry of Health).
Florida CE statement
Approved for 45 contact hours (4.5 CEU) — General Hours, PT & PTA.
CE Broker Tracking 20-1318645 · FPTA Approval CE25-1318645 · Effective 01/01/2025 – 12/31/2025.
Renewal confirmed for 2026 and beyond, so your credits remain valid regardless of when you enroll.
FPTA disclaimer: "Accreditation of this course does not necessarily imply the FPTA supports the views of the presenter or the sponsors."
Further study
AIFiMM continues to expand its research and educational activities on systemic biomechanics.
For scientific articles, theoretical insights, and comparative analyses related to this model, visit the Scientific Articles section on our website.
It provides a continuously updated reference for professionals wishing to explore the theoretical foundations and clinical applications of systemic biomechanics.
Visit the Scientific Articles section
Available courses
Systemic Musculoskeletal Biomechanics
✅ How to Enroll in the Course
Follow these simple steps to complete your enrollment in the online course:
1️⃣ Click on “Request enrollment”
You’ll be redirected to a page summarizing the key details of the course (duration, price, structure, etc.).
2️⃣ Click on “Proceed with enrollment”
You’ll be taken to the registration page on the AIFiMM platform.
You will need to:
-
Enter a valid email address (a verification check will be performed)
-
Choose a personal password that you will use to log in to your private area
3️⃣ Complete your registration
Fill in the required personal and professional information, then click “Confirm registration”.
🔐 Registration is necessary to access the final enrollment page.
4️⃣ Access the final enrollment page
Once registered, you will be able to:
-
💳 Choose your payment method: credit or debit card via Stripe
-
💰 Choose how you want to pay: in a single payment or in installments
5️⃣ Confirm your enrollment
Check the box to accept the terms and conditions, then click “Confirm enrollment” to finalize your registration.
❓ Need help?
If you encounter any issues during the enrollment process or don’t receive the confirmation email, please contact our technical support:
📧 info@lysla.it
(Answered by Carmen Ghirardi, IT manager at AIFiMM)
We’ll be happy to assist you!
⚠️ Important Note on Installment Payments
Installments are charged monthly on a fixed schedule.
Access may be suspended if payments are missed.
The certificate will be issued only after full payment is completed.
🎓 Credits Reminder
-
CEU (USA) – This course is approved by the Florida Board of Physical Therapy Practice for 45 contact hours (4.5 CEU) — General Hours, PT & PTA.
CE Broker Tracking 20-1318645 · FPTA Approval CE25-1318645
Valid Jan 1 – Dec 31, 2025 · Renewal confirmed for 2026 and beyond. -
CPD (UK & International) – This course is accredited by the CPD Certification Service (Provider No. 21418) for 38 CPD hours.
Recognized internationally for Continuing Professional Development.
Copyright © 2025 AIFiMM Formazione Mézières Provider E.C.M. n. 1701. All rights reserved.